
One of the most common sleep movement disorders explained.
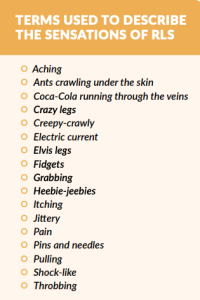
Restless legs syndrome (RLS) is a sensorimotor neurologic disorder with a profound impact on sleep. The difficult-to-describe sensations (sensory) and urge to move (motor) occur most often during rest or inactivity, primarily in the evening and at night, and are relieved by movement. Once thought to be rare, RLS is now understood to be fairly common, affecting almost 3% of adults with moderate to severe symptoms at least 2 nights a week.
 RLS can be primary, meaning that it has no known cause other than perhaps a genetic predisposition, or it can be secondary. Secondary RLS, sometimes called comorbid RLS, is associated with another condition, most commonly with iron deficiency, end-stage kidney disease, or pregnancy. Cardiovascular disease and Parkinson’s disease may also be comorbid conditions, but the science behind those is a little less clear.
RLS can be primary, meaning that it has no known cause other than perhaps a genetic predisposition, or it can be secondary. Secondary RLS, sometimes called comorbid RLS, is associated with another condition, most commonly with iron deficiency, end-stage kidney disease, or pregnancy. Cardiovascular disease and Parkinson’s disease may also be comorbid conditions, but the science behind those is a little less clear.
AGE OF ONSET OF RLS
RLS has a bimodal distribution of onset, meaning that there are two peak times when most people develop RLS—one peak is about age 20 and the other is in the mid-40s. In younger people, the likelihood is greater that they will have another family member with RLS, as compared with people older than 30. This has led researchers to speculate that heredity (genetics) might play a role in people with RLS who have a younger age at symptom onset.
DIAGNOSIS OF RLS
There is no specific blood or imaging test to diagnose RLS. Instead, the gold standard is a clinical interview. Without that interview to rule out RLS mimics, many other conditions fulfill the four original diagnostic criteria for RLS, which led to an overestimation in epidemiologic studies of the number of people who actually have RLS. However, when knowledgeable clinicians ask appropriate questions to tease out the presence of those RLS mimics, a more accurate diagnosis can be made; therefore, the fifth criterion was added to the diagnostic criteria in 2014. When the diagnosis is not clear through the interview, clinicians may order laboratory or imaging tests to rule out other conditions.
“Once thought to be rare, RLS is now understood to be fairly common, affecting almost 3% of adults with moderate to severe symptoms at least 2 nights a week.”
TREATMENT OF RLS
The Medical Advisory Board (MAB) of the RLS Foundation published an algorithm, or step-by-step guide, on treating RLS in 2004, and an update in 2013. Because new information has come to light, the Board updated the algorithm again in 2021, offering unique insights into a variety of RLS treatments. John Winkelman, MD, PhD, Chief , Sleep Disorders Clinical Research Program at Massachusetts General Hospital; Professor of Psychiatry, Harvard Medical School; and a member of the Foundation’s MAB, has provided some key points from the new algorithm.
NONPHARMACOLOGIC THERAPY OF RLS
 Nonpharmacologic treatment may be helpful for mild symptoms or for reducing more severe symptoms. As has long been the case, the Board members recommend beginning with an assessment of each patient’s current medications, both over-the-counter and prescribed, and identifying any that may be exacerbating RLS symptoms. If possible, medications that worsen the RLS should be discontinued or changed to another drug that is less likely to affect RLS symptoms. In addition, every patient’s iron stores should be measured with a full serum iron panel. Inadequate stores should be replenished with either oral or intravenously administered iron, as appropriate. People with RLS may find that not consuming caffeine or alcohol may help to reduce their symptoms, as may engaging in mentally alerting activities during periods of inactivity, such as while a passenger on an airplane, which often strikes dread in the hearts of people with RLS. In the case of flying, taking a flight earlier in the day rather than in the evening may also help with reducing symptoms.
Nonpharmacologic treatment may be helpful for mild symptoms or for reducing more severe symptoms. As has long been the case, the Board members recommend beginning with an assessment of each patient’s current medications, both over-the-counter and prescribed, and identifying any that may be exacerbating RLS symptoms. If possible, medications that worsen the RLS should be discontinued or changed to another drug that is less likely to affect RLS symptoms. In addition, every patient’s iron stores should be measured with a full serum iron panel. Inadequate stores should be replenished with either oral or intravenously administered iron, as appropriate. People with RLS may find that not consuming caffeine or alcohol may help to reduce their symptoms, as may engaging in mentally alerting activities during periods of inactivity, such as while a passenger on an airplane, which often strikes dread in the hearts of people with RLS. In the case of flying, taking a flight earlier in the day rather than in the evening may also help with reducing symptoms.
PHARMACOLOGIC THERAPY FOR RLS
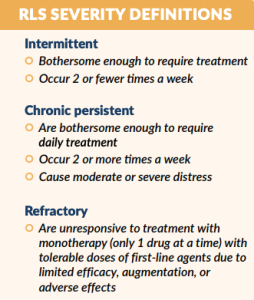
Starting treatment with medication first involves determining whether the symptoms are intermittent, chronic persistent, or refractory.
INTERMITTENT RLS THERAPY
Because intermittent RLS affects people on 2 or fewer days per week, they don’t need pharmacologic treatment every night. In this case, people may take medications such as levodopa, a benzodiazepine (a sleeping pill), or a low-dose opioid (for example, tramadol or codeine) only as needed. Augmentation, as discussed in the following section, can occur with levodopa, so it is important to keep the dose as low as possible. Both benzodiazepines and opioids should be used with caution, paying attention to potential side effects.
CHRONIC PERSISTENT RLS THERAPY
A key point highlighted in the newest algorithm is a change in consensus on first-line treatment of moderate to severe (chronic persistent) RLS. The first medications approved by the US Food and Drug Administration (FDA) to treat RLS were the dopamine receptor agonists—pramipexole, ropinirole, and later, rotigotine. All of these drugs have been found to be beneficial in relieving the symptoms of RLS for most people; however, over time, their use often produces what medical professionals term augmentation (see page 16 for definition of augmentation). Because of this, the Board now recommends starting treatment of RLS with drugs called alpha-2-delta ligands. These include gabapentin, pregabalin, and gabapentin enacarbil, with gabapentin enacarbil having FDA approval for the treatment of RLS and the others used off-label. If a person cannot take an alpha-2-delta ligand or their symptoms are not responsive to this class of drugs, a dopamine receptor agonist can be used, but the dose should be kept as low as possible.
A recently published study that examined a prescriptions database in the United States found that 60% of the 670,000+ patients identified as having RLS are currently being treated with dopaminergic agents. Twenty percent of those, approximately 75,000 people, are being prescribed doses of dopaminergic agents above FDA- and guideline-recommended doses, with half of those prescribed doses at 150% or more of FDA- and guideline-recommended doses. According to Dr. Winkelman, “Dopaminergic agents have been used as first-line therapy for many years for RLS, but we now recognize that the high risk of augmentation outweighs their short-term clinical benefits. The large number of patients who are prescribed doses that are well above FDA-recommended doses is discouraging and an indication that alternative approaches need to be instituted that will allow patients to reduce or discontinue their dopaminergic medications. Using such high doses of dopaminergic agents is like throwing gasoline on the fire of RLS.”
REFRACTORY RLS THERAPY
For improving RLS symptoms and thus sleep and quality of life, the RLS Foundation algorithm recommends considering the use of opioids in people with refractory RLS. Because RLS symptoms are present for at least 12 hours per day in most people with refractory RLS, long-acting opioids (such as methadone, buprenorphine, and extended-release oxycodone) are the most commonly prescribed opioid medications for RLS. People with RLS who take opioids typically do not experience dose-escalation, (that is, a need for higher and higher doses), and, in RLS patients who do not have a history of abuse, misuse (that is, taking the drug in a manner not prescribed) is uncommon. Clinicians should use caution but should not withhold this treatment from appropriate patients. The choice of which opioid to use depends on the patient’s symptoms, comorbid conditions, and other factors.
RLS DURING PREGNANCY AND WHILE BREASTFEEDING
 Pregnancy may be a particularly challenging time for women with RLS, and RLS may also appear for the first time during pregnancy. RLS is fairly common during pregnancy: research that pooled the results of 27 different studies of RLS during pregnancy found that rates in the trimesters were 8%, 16%, and 22%, respectively. Women who develop RLS during pregnancy are at increased risk for having RLS symptoms later in life, but, for most women, RLS resolves with delivery.
Pregnancy may be a particularly challenging time for women with RLS, and RLS may also appear for the first time during pregnancy. RLS is fairly common during pregnancy: research that pooled the results of 27 different studies of RLS during pregnancy found that rates in the trimesters were 8%, 16%, and 22%, respectively. Women who develop RLS during pregnancy are at increased risk for having RLS symptoms later in life, but, for most women, RLS resolves with delivery.
As in other cases of RLS, maintaining adequate iron stores in pregnancy can help to relieve symptoms. When nonpharmacologic therapy and iron replenishment do not control symptoms, the recently published algorithm from the RLS Foundation’s MAB recommends using the lowest possible doses of medication, preferably on an as-needed basis, in only the second and third trimesters. Clonazepam, levodopa, and low-dose oxycodone may be used with caution, but the patient and clinician should discuss the risk-benefit profile of each drug and should consult with the obstetrician.
In the previously mentioned study of RLS in pregnancy, 4% of women continued to have RLS in the postpartum period. For these women with RLS who choose to feed their babies with breastmilk (ie, lactate), any dopamine drugs (eg, levodopa and dopamine receptor agonists) should be avoided because they inhibit lactation. Treatment options during lactation include clonazepam, gabapentin, and tramadol. Again, caution should be exercised because of side effects of these medications, particularly sedating effects.
CONCLUSION
As researchers have uncovered more clues to the cause of RLS and as current treatment options have been available for longer periods of time, our understanding of RLS and its treatment have changed. More effective treatments have become and will continue to become available. Clinical trials of newer agents and studies of currently available drugs in adolescents are ongoing. Patient participation in these trials and clinicians conducting other research are necessary to continue to discover the answers to the mystery of RLS.
______________________________________________________________________________________________________
Catherine Friederich Murray, MNLM earned her BS in biomedical communications at the University of Minnesota and her masters in nonprofit leadership and management from Arizona State University. She has worked as a writer and editor in sleep for more than two decades and led two sleep-related patient advocacy organizations during that time.
References:
- Garcia-Borreguero D, Silber MH, Winkelman JW, et al. Guidelines for the first-line treatment of restless legs syndrome/Willis–Ekbom disease, prevention and treatment of dopaminergic augmentation: a combined task force of the IRLSSG, EURLSSG, and the RLS-foundation.Sleep Med.2016;21:1-11.
- Allen RP, Picchietti D, Hening WA, Trenkwalder C, Walters AS, Montplaisi J. Restless legs syndrome: diagnostic criteria, special considerations, and epidemiology.Sleep Med.2003;4(2):101-119.
- Allen RP, Walters AS, Montplaisir J, et al. Restless legs syndrome prevalence and impact: REST general population study.Arch Intern Med.2005;165(11):1286-1292.
- Trenkwalder C, Allen R, Högl B, et al. Comorbidities, treatment, and pathophysiology in restless legs syndrome.Lancet Neurol.2018;17(11):994-1005.
- Whittom S, Dauvilliers Y, Pennestri MH, et al. Age-at-onset in restless legs syndrome: a clinical and polysomnographic study.Sleep Med.2007;9(1):54-59.
- Allen RP, Picchietti DL, Garcia-Borreguero D, et al. Restless legs syndrome/Willis-Ekbom disease diagnostic criteria: updated International Restless Legs Syndrome StudyGroup (IRLSSG) consensus criteria–history, rationale, description, and significance.Sleep Med. 2014;15(8):860-873.
- DelRosso LM, Ferri R. Restlesslegs syndrome and periodic leg movements of sleep.In: Gozal D, Kheirandish-Gozal L, eds. Pediatric Sleep Medicine: Mechanisms and Comprehensive Guide to Clinical Evaluation and Management. Springer International Publishing; 2021:395-401.
- Kwatra V, Khan MA, Quadri SA, Cook TS. Differentialdiagnosis and treatment of restless legs syndrome: a literature review.Cureus. 2018;10(9):e3297.
- Silber MH, Ehrenberg BL, Allen RP, et al. An algorithm for the management of restless legs syndrome.Mayo Clin Proc.2004;79(7):916-922.
- Silber MH, Becker PM, Earley C, Garcia-Borreguero D, Ondo WG, Medical Advisory Board of the Willis-Ekbom Disease F. Willis-Ekbom Disease Foundation revised consensus statement on the management of restless legs syndrome.Mayo Clin Proc.2013;88(9):977-986.
- Silber MH, Buchfuhrer MJ, Earley CJ, et al. Themanagement of restless legs syndrome: an updated algorithm.Mayo Clin Proc. 2021;96(7):1921-1937.
- Anguelova GV, Vlak MHM, Kurvers AGY, Rijsman RM. Pharmacologic andnonpharmacologic treatment of restless legs syndrome.Sleep Med Clin. 2018;13(2):219-230.
- Garcia-Borreguero D, Silber MH, Winkelman JW, et al. Guidelines for the first-line treatment of restless legs syndrome/Willis-Ekbom disease, prevention and treatment of dopaminergic augmentation: a combined task force of the IRLSSG, EURLSSG, and the RLS-foundation.Sleep Med.2016;21:1-11.
- Winkelman JW. High national rates of high-dose dopamine agonist prescribing for RLS.Sleep.2021.
- Chen SJ, Shi L, Bao YP, et al. Prevalence of restless legs syndrome during pregnancy: A systematic review and meta-analysis.Sleep Med Rev.2018;40:43-54.